
Case-Report | DOI: https://doi.org/10.31579/2692-9392/007
*Corresponding Author: Lee Eng Kiang, Senior Consultant Intensive Care Medicine Ng Teng Fong General Hospital.
Citation: Lee Eng Kiang. (2020) Suicide from a Cerbera odollam kernel J. Archives of Medical Case Reports and Case Study. 3(1); DOI:10.31579/2692-9392/007
Copyright: © This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 12 November 2019 | Accepted: 20 December 2019 | Published: 02 January 2020
Keywords: suicide; pong pong; cerbera odollam; digoxin
We report the case of a 22 year-old female patient who died 24 hours after consuming 2 seeds of the mangrove plant Cerbera odollam, locally known as the Pong pong tree from fatal dysrhythmia. This fruit is responsible for a lot of suicidal deaths in Kerala, India but rarely in Singapore1. These seeds contain active cardiac glycosides similar to digoxin which can result in fatal dysrhythmias and hyperkalaemia.
Suicide is the leading cause of death in Singapore for the age group ranging from 10 to 29 years. There are a total of 361 in 2017 and a male predominance of 66% of all the deaths.
The unfortunate patient is a 22 year old female who was known to have mood disorders and also depression for 4 years. She had been on regular follow ups at the psychiatric and psychological clinics and previous suicidal attempts. She admitted that she had taken 2 seeds of the Cerbera odollam, figure 1 or locally known as the Pong Pong tree on the night prior to the admission to the emergency department. She actually purchased the seeds via the internet after reading about the suicidal effects of the seeds.

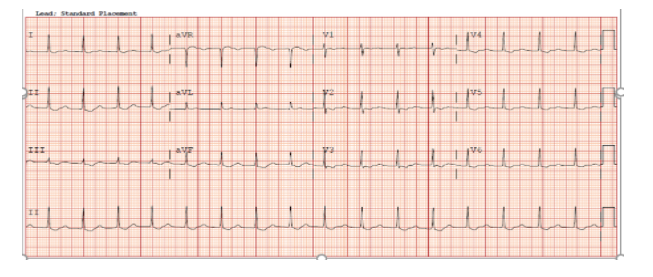
She was in atrial fibrillation with a rate above 100 per minute and her blood pressure was 120/80 mmHg when she first arrived in the emergency department(ED) approximately 12 hours after eating these seeds. Subsequently in the ED she had repeated episodes of vomiting and complained of acute abdominal pain and oral charcoal was not given. The first 12 leads ECG done showed a rhythm with an atrial fibrillation with a rate of 100 to 110 per minute, (figure 2).

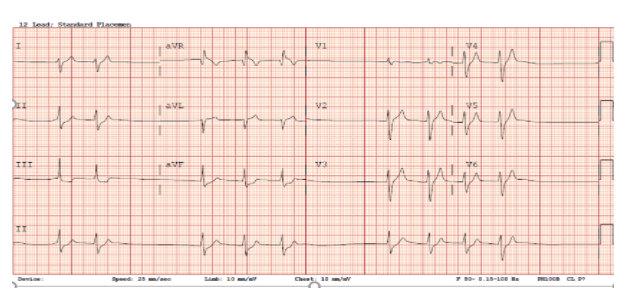
The hospital’s laboratory was unable to measure cerberin level which is a type of cardiac glycosides. The digoxin level was done as a surrogate marker of cerberin toxicity. She was given 200mg of digoxin specific immune Fab fragments after the level of Potassium came back as 5.3 mmol/l and her digoxin level was 1 ng/ml. She responded to the treatment and got back into sinus rhythm and was 2 hours post admission as seen in figure 3 ECG.
Over the next one hour, there was a change in her pulse rate as the subsequent ECG showed brady arrhythmia with prolonged PR interval atrial fibrillation. Her systolic blood pressure had also decreased from above 120mmHg to about 100 mmHg. Her Potassium level also came back as 9.8 mmol/l and she was immediately administered with intravenous calcium glucoronate, insulin and dextrose and atropine for the brady arrhythmia as seen in figure 4 ECG. She was referred to the ICU for urgent renal dialysis in view of the rising Potassium and drop in blood pressure.
She was persistently in bradycardia despite a total of 2.4 mg of atropine given intravenously. The dialysis catheter was inserted immediately and continuous renal replacement therapy was started as soon as she reached the ICU. She also received another 200mg of of digoxin specific immune Fab fragments and intravenous lipofundin as well. The patient however didn’t improve and instead she showed widened QRS complexes which progressed to ventricular fibrillation prior to asystole, figure 5. She received 2 full hours of external cardiac compression and ventilator support before she was pronounced dead. This patient developed clinical evidence of arrhythmia despite a total of 400 mg digoxin specific immune Fab fragments, 500ml of lipofundin 20% and hemodialysis. All of which didn’t manage to reverse the toxicity of the cardiac glycoside from the kernels.

It has been to my best knowledge that a suicidal case involving the kernel of Cerbera odollam has never been reported in Singapore.
For generations mothers in Singapore have warned their children about consuming this Pong Pong fruit but the toxicity of the kernel was never highlighted. These seeds contain active cardiac glycosides, cerberin, cereberoside and odollin and can result in fatal dysrhythmias similar to digoxin toxicity.
This patient was able to obtain information about this toxic fruit and was also able to make her purchase via the internet which was marketed as a suicidal fruit.
The patient mentioned in our case report had similar symptoms and clinical presentations as other patients mentioned in other case reports [2,3,4,5]. She presented with symptoms of abdominal and vomiting and subsequently arrhythmia and hyperkalemia. She also collapsed 24 hours after eating the seed despite all the measures taken to reduce the toxicity of the cardiac glycoside. As in other case reports, hyperkalemia is associated with very high mortality and in this case may have precipitated the bradycardia and subsequent ventricular fibrillation. The measured digoxin of 1 ng/ml may not truly reflect the severity of cardiac glycoside toxicity in this patient even though in other series of poisoning all patients who died had a digoxin level above 1.0 ng/ml. The only method of identifying cardiac glycoside is by thin-paper chromatography and unfortunately this may not easily available in most general hospitals.
It is a challenge managing this patient who had gone into cardiac arrest as the underlying toxins cannot easily cleared from the body. As highlighted the actual dosage of anti-digoxin immune Fab is unknown for cardiac glycosides as the current dosing is based on that digoxin measured in the plasma. Intravenous liopfundin 20% was also mentioned in other case reports as a possible antidote and we had also attempted to use it in this patient but unfortunately it was not shown to be effective [4,5,6,7] It was initially used for treating local anaesthetic toxicity such as bupivacaine but its usage as an antidote has been expanded to other drugs but at this stage no strong recommendation for digoxin toxicity has been established.
The use of transcutaneous pacing was considered but the inhibition of the Na-K ATPase pump may cause poor nerve conduction and render it ineffective.
ECMO was considered as a possible temporizing measure but the plan was abandoned. This is because the patient had received intravenous lipofundin 20% infusion which may increase fat deposition in the membrane of the VA-ECMO and increased blood clot formation [8].
Ingestion of the Cerbera odollam seeds can cause fatal cardiac glycoside toxicity. Unfortunately, this seeds are easily available in Singapore and also available via internet purchase. It is also sold as a form of decorative ornaments.
The other types of related cardiac glycoside toxicity can also arise from plants such as yellow oleander, foxglove and herbal dietary supplements [1,2,3]
Cardiac glycoside binds to and inhibits cellular Na/K-ATPase (the sodium/potassium pump). This pump transport sodium out of the cell and potassium into the cell necessary for action potentials in exciting nerves and muscles. When the pump is blocked, sodium accumulates inside the cell and this leads to an increase of intracellular calcium and extracellular potassium. The increase of calcium leads to an increase in heart contractility. In a normal healthy patient this forces the heart to work harder and can lead to arrhythmia. Hyperkalaemia can also precipitate brady arrhythmia which is highlighted in this case.
Digoxin specific Fab fragments are digoxin specific antibody Fab fragments which are purified from sheep plasma and they bind rapidly to digoxin. Fab fragments also diffuse into the interstitial space where they bind to digoxin in the tissues and as a result, the free digoxin level is rapidly reduced, creating a favorable concentration gradient for the efflux of digoxin out of the cells and into the extracellular fluid where it binds to digoxin specific fragments. The bounded digoxin cannot bind with inhibitory site on the alpha subunit of Na-K ATPase pump in the cell wall.
The molecular structures of the cardiac glycoside, ceberin and digoxin showed a lot of structural differences and these differences may be the cause why the cardiac glycoside may not bind as well as digoxin to the anti-digoxin immune Fab, figure 6. The effectiveness of the antidote on cerberin has never been well studied or reported.
The pharmacokinetic and dynamic of these cardiac glycosides from these kernels are not well studied. Oral absorption may be enhanced or delay depending whether it was taken with or without any other food. It is also not known if all the different cardiac glycosides have the same toxicities.
Cardiac glycoside is associated with high mortality as seen in the other case reports and also in our patient. More studies need to be done about these various cardiac glycosides and also their pharmacodynamics and pharmacokinetic properties. More education and preventive measures must be in place to prevent further incidence of such poisoning in the future.
The post mortem report was not available at the point of this report and it may provide further information about the structural changes associated with the myocardium as a result of the cardiac glycoside toxicity.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
